History of Porcelain Veneers
Often considered the penultimate of cosmetic dentistry, dental porcelain veneers are a powerful way to idealize nearly all smiles. Historically, veneers were not always comprised of porcelain—in fact the inventor of veneers, Charles Pincus, started placing acrylic laminate veneers in the 1930’s on patients to hide their missing or broken teeth when they were acting (he was a California dentist). The adhesive technology was not in place at that time for these to be considered true dental restorations, however they did serve the purpose of establishing the foundation for what today is considered the highest form of cosmetic dentistry. Today, dental veneers are made from a variety of materials, including composite resin, porcelain, zirconia, and even acrylic.
In the 1980’s porcelain veneers transitioned into what today are considered long-lasting and esthetic restorations. Adrian Jurim applied for and received a 1986 patent for his idea of the etched porcelain laminate veneer. Etching porcelain with hydrofluoric acid is a critical step in adhering porcelain, with a relatively strong bond, to modern dental adhesive materials. Because dental adhesive materials can obviously bond to tooth structure, the porcelain etching concept was a critical step for this restorative modality. During the 1980’s veneers were predominantly comprised using refractory techniques where a thin metal foil is placed on the tooth models and the porcelain is stacked. This method, often referred to as powder-liquid or feldspathic veneers, enabled a talented technician to create absolutely beautiful veneers. In the paragraphs that follow, the various types of veneers available are discussed in terms of material type with the pros and cons of each type mentioned.
Feldspathic Porcelain Veneers

Examples of Feldspathic Porcelain Systems from Ceramco and Noritake
The degree of difficulty is extremely high with feldspathic porcelain veneers, and these veneers are extremely fragile prior to bonding. In addition, the fit of the veneers is not as ideal as some of today’s alternative options. Nevertheless, feldspathic porcelain veneers are still used today, and are absolutely beautiful in their appearance. The esthetic control a technician has is outstanding, as the entire veneer is literally built by hand with various ceramic “powders” that a liquid is applied to in order to create the color scheme and effects that are desired. For this reason, this class of veneers can be referred to as “powder-liquid” veneers. A similar technique is used when making a porcelain-fused-to-metal crown, however there is no metal coping (framework) used to stack the porcelain to. In the right hands, no veneer material can be made that is more beautiful than feldspathic porcelain veneers, however today this is a dying art due to the labor and time involved in their fabrication and compromised strength. Once bonded in place, a feldspathic veneer is quite strong, however prior to adhesive placement, these veneers can break easily when they are held, tried onto the teeth, or dropped on a countertop or floor.
Composite Resin Veneers
Dentists use composite resin bonding material to fill cavities, but when applied to the front teeth, many doctors and patients refer to this technique as “bonding.” Composite bonding can be completed on the front teeth as a cost-effective alternative to porcelain veneers. The composite resin can be fabricated either by a dentist placing material directly onto a tooth or teeth (chair-side composite laminate veneer) or by a laboratory technician (laboratory-fabricated composite laminate veneer). If the teeth are prepared first, by removing stains, smoothing chipped surfaces, or pulling teeth back that are out of the arch form, composite resin can be applied to create beautiful veneers. Without preparation of the teeth, it is difficult to make pre-veneer fully-contoured teeth appear natural, and they tend to look bulky.

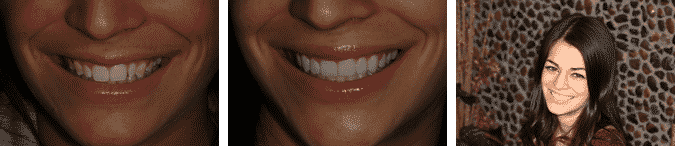
Example of a Chair-Side Composite Laminate Veneer. Actual cosmetic patient of Brent Engelberg, D.D.S.
Issues or concerns with composite veneers are limited strength of the plastic filling material and its tendency to stain (especially over time) or have pitting on the surface of the veneers caused by air incorporation. In addition, the technique sensitivity of the process is high both for the adhesion of the veneer bonding material to the tooth as well as achieving a great cosmetic result. Most dentists tend to use one or perhaps two shades of composite resin with these veneers. The reality is that the best ceramists might utilize over ten different shades of porcelain to alter the hue, value, and chromatic characteristics of high-end veneer restorations. When having composite veneers placed, a mix of available composites possessing different colors, translucencies, and opacities should be correctly incorporated into the restorations to yield an ideal cosmetic result—a technique that most dentists do not care to spend the time to master. Typically, it will take just as much if not more time to correctly place a highly cosmetic direct composite veneer then it would take to have two appointments in which the laboratory would fabricate an all porcelain veneer. The potential for a lower cost composite veneer is often realized in the form of a monochromatic and less esthetic restoration.
Pressed Porcelain Veneers
Veneers can be made by utilizing a technique similar to the lost wax technique that has been used in metal working and jewelry making for centuries. Typically, a block or ingot of porcelain material is melted or heated to a honey-like consistency, and pressed or injected into an investment housing around an empty space that was filled with a wax template of a veneer. The wax is melted and removed prior to pressing the porcelain into the space, and the surrounding matrix is divested to reveal the formed veneers. This technique leaves a very strong and accurate fitting veneer as a result. The materials used for this technique are varied, and brand names include Empress by Ivoclar Vivadent, Authentic by Jensen Dental, and recently IPS e.max by Ivoclar Vivadent to name a few. Dr. Brent Engelberg, a cosmetic dentist in the Chicago, Illinois suburbs, uses pressed porcelain veneers made by Brad Jones of Boise, Idaho, in the overwhelming majority of his cosmetic dentistry cases.

An example of highly esthetic pressed porcelain veneers in a dramatic smile makeover. Actual Cosmetic Patient of Brent Engelberg, D.D.S.

Ceramist Brad Jones layering porcelain on a cosmetic case for one of Dr. Engelberg’s Chicago dental patients. Actual Cosmetic Patient of Brent Engelberg, D.D.S.
Pressed veneers are made and either stained and glazed, or made by a cutback and layering technique. The former technique requires minimal completion time and does not alter the strength of the restoration once it has been pressed. The later technique is much more labor intensive, can alter the strength of the porcelain, and yields a much more esthetic result. When a cutback is done, the biting edges of the anterior teeth are usually removed by the ceramist, and multiple layers of porcelain are stacked and fired in a sequence with the goal of recreating the natural layers of a tooth. In addition, this technique allows for detailed and customized shading, and incisal edge details such as translucency and the creation of halo’s and color seen in natural teeth. The cutback and layer technique is considered to be the highest level of cosmetic dentistry a patient can receive with pressed veneers, and is a technique mastered by very few ceramists in their career. The amount of time it takes to properly cutback and layer a smile design case in one arch can vary from a full day to over a week depending on the ceramist and esthetic characteristics they desire to create.
CAD/CAM Porcelain Veneers
The CEREC or E4D systems offer CAD/CAM porcelain veneers as part of their system. CAD/CAM systems operate with advanced technology that enables a dentist to scan a tooth preparation (in lieu of an impression) digitally, and then design a veneer, inlay, onlay, or crown. With these machines, the veneer would be made from a solid block of porcelain. This block is milled by a machine to replicate what had been designed by the computer software. The blocks are made by a variety of companies, however Ivoclar Vivadent holds the dominant market share. 3M is also a major manufacturer of these blocks. The issue with the blocks is that they are mostly a solid block of one color, which leads to unesthetic and monochromatic veneers. There are blocks that are graded from top to bottom within a shade family, and the block is milled with the biting edge to be more clear and the gum edge to be warmer in color.
Veneers made with CAD/CAM technology are made of either all porcelain or variously composed composite blocks. Ivoclar Vivadent’s market domination of the blocks indicates that IPS e.max is the fastest growing porcelain material selected by dentists for use in the mouth. When e.max CAD blocks are used, the strength is in the 360 mPA range. When e.max Press is used when making veneers, the strength is much higher as a result of the formation of the porcelain. CAD porcelain blocks of e.max are made from a heating process and the crystals grow randomly, effectively rendering the porcelain a bit weaker. With other types of porcelain blocks, the case has been made that the blocks are so homogenous that the porcelain is stronger than if the porcelain was stacked by hand.
No matter the viewpoint, it is clear that CAD/CAM technology is here to stay, and that it will continue to change dentistry. The fact is that in-office CAD/CAM technology with CEREC or E4D restorations are made by dentist and their staff. Designing a well-contoured veneer is hard enough for a lab technician, let alone a dentist or dental assistant. In addition, these restorations are typically polished only, or lightly stained. The product is an average, at best, esthetic result assuming the veneers are properly shaped. The majority of CEREC users report that they use their machines for posterior (back) teeth only, since these restorations cannot easily be seen by the patient, friends, or family. Very few clinicians are able to place an ideal cosmetic CAD/CAM veneer that is highly esthetic without substantial manipulation of the restoration after it has been milled, which eliminates the main benefit of this technology: speed. Currently, the reality of CAD/CAM veneers is that they are not nearly as esthetic as feldspathic veneers, pressed cutback and layered veneers, or even well-made composite resin veneers.
Zirconia Veneers
Zirconia veneers are a newly emerging material for restoring teeth. Bonding zirconium-based restorations cannot be done with the same methods of traditional glass-porcelain.25, 26 Zirconia (ZrO2) is a silica-free, acid-resistant, polycrystalline ceramic that does not contain amorphous silica (SiO2), making it ineffective to traditional glass-etching treatments such as hydrofluoric acid (HFl) followed by silane application.20 The premise behind using Zirconia as a restorative material is that it is extremely strong—over 1,100 mPa, which is more than double the strength of pressed e.max for example. However it is not as esthetic as other materials used for crowns and veneers because of its inherent opacity.27 There are promising techniques to bond zirconia to teeth,21-24 however with the current esthetic limitations, zirconia is not today considered to be an ideal material for an esthetic restoration. Layering zirconia makes it more cosmetically appealing; however this adds bulk, and therefore greater tooth reduction requirements which are undesirable.
Minimal Preparation Veneers and No Prep Veneers (Prepless Veneers)
No-Prep or Prepless veneers are a hot topic in dentistry today. There are several reasons for the increase in popularity of prepless veneers, including patient demand for a seemingly conservative and reversible dental procedure that is cosmetic. Dentists have also long desired a way to simplify the process of preparing veneers as well as being conservative to tooth structure—what better way than to eliminate the preparation of a tooth or teeth altogether! One large corporate dental laboratory markets Lumineers (their brand name, like Kleenex is a name brand of tissue) in many print and electronic advertising campaigns. In addition, Durathins, Emprathins, and other brand name prepless veneers are on the market today. While the aforementioned products are brand-name prepless veneer options, any dental laboratory can make a prepless veneer.
Prepless Veneers (No Prep Veneers)

Prepless veneers require a talented dentist-ceramist combination to look natural and blend into the dentition.

A completed prepless veneer case by Dr. Engelberg that disappears in the mouth–ten teeth in this photo have veneers in place.
A prepless veneer is when a dentist simply takes an impression of unprepared teeth and sends this to a laboratory for veneers to be made. The lab fabricates additive veneers on the model of the teeth that are to be enhanced, and sends this back to the dentist who bonds the veneers into place. Dr. Engelberg and master ceramist Brad Jones have devised their own technique for this type of veneer, called “Prep-Less” where either no preparation is performed on the teeth, or a combination of no prep veneer and minimal preparation veneer is performed as needed.
In the example case shown, Dr. Engelberg slightly prepared 4/10 teeth, 2/10 teeth were lightly polished, and the remaining 4/10 teeth were not prepared at all. The reality is that this procedure is case specific in its application. The case shown turned out to be beautiful, however in order to do this the upper right canine had to be shortened (it was too low), so totally prepless was not an option. However, the lateral incisors were peg in nature, and needed mainly to have porcelain added to them (basically prepless). A combination case is usually performed in these situations for an ideal result.
The goal of cosmetic cases should be twofold: preservation of tooth structure as well as a highly aesthetic result. The more conservative the preparation, the safer it is for the pulpal status of a tooth. In addition, the more enamel present on a tooth, the better the bond of the veneer to a tooth, therefore no prep veneers or “prep-less” veneer combination cases should be employed whenever possible.
Before smile photo of a great candidate for prep-less porcelain veneers. Note the lower canine on the patient’s left side needing gum alteration as well as minimal preparation of the length.
Prepless Veneer Glamour Smile” with the caption, “The happy patient with a beautiful smile and extremely conservative cosmetic dentistry.
After smile photo of the same patient after prep-less porcelain veneers by Dr. Engelberg with the teeth having more ideal proportions.
Minimal Preparation Veneers
A minimal preparation veneer is basically the same in format, although a dentist will round a sharp corner, remove a portion of a tooth that is flared, or perhaps have the lab dictate a couple of spots to lightly touch up in the mouth prior to seating the veneers.
The concepts of no prep and minimal preparation veneers are not new. In fact, the first veneers placed were often done with minimal or no preparation of tooth structure and bonded to nearly 100% enamel. This was a great idea as the highest bond strengths were then, and still are, to enamel. What these early cases did, however, was typically bulk up the teeth already present in the mouth. In cases where there is limited spacing, adding porcelain is a great idea. In cases where the teeth are reclined, or pointed inward toward the tongue, adding porcelain can produce a nice result. There are several situations where some teeth do not need to be prepared at all, while others in the same patient do need to be prepared, and this is something that should be determined by a dentist prior to starting a case—not the laboratory once the case has arrived. Finally there are many case examples where the teeth must be prepared, meaning prepless veneers are not an option. For example, if tooth decay is present, it must first be removed prior to placing veneers.

An example case where prepless (or even minimal prep) veneers are not an option; tooth decay, pre-existing bulky minimal preparation veneer restorations, and actual tooth position do not allow it. This highly esthetic result was only achieved with some tooth preparation. Actual Cosmetic Patient of Brent Engelberg, D.D.S.
The cosmetic reality is that many patients who are seeking veneers have additional concerns with their teeth that cannot be addressed by performing “additive veneers” only. Patients with healthy teeth that are in proper alignment and no dental work that needs to be replaced are good candidates for prepless veneers—however these patients usually do not have a desire for veneers since their teeth look great! If you can simply whiten your teeth (without veneers) no dentist can argue that veneers of any type are a better choice for treatment. The best treatment is no treatment is applicable in all cases, and this applies to veneers of any kind.
Lumineers
This is a brand name for a widely marketed brand name veneer made by a specific dental lab, DenMat. According to their website, Lumineers are unlike traditional veneers as there are no shots, no drilling of sensitive tooth structure, and no pain. They’re even reversible, so you have nothing to lose and a beautiful smile to gain. This is great marketing, however in practice, Lumineers are a mass marketed brand of veneer that can only be made by one dental lab–with a wide variety of technicians making these veneers. The experience level of the technicians varies, and very few of them if any are master ceramists. Nearly no high end cosmetic dentists place lumineers routinely in their practices, as they are simply less esthetic than quality veneers made by an artistic ceramist working as a member of a team along with the dentist and patient.
In addition, the claim that Lumineers are reversible is not accurate—while in some cases these veneers can be done with no preparation, when finishing the veneers at the time of seating, tooth structure is permanently removed. In addition, to remove adhesively bonded veneers of any type always involves the removal of some tooth structure—the resin cements alone permeate into the tooth surface irreversibly. Finally, these cases are limited by the same rules governing the placement of minimal preparation veneers as described above. In cases where the teeth have spaces or are tucked in, additive veneers like Lumineers can possibly be performed with good clinical results. However, in cases where the teeth are overlapped, crooked, flared out, contain decay, contain fillings, bonding, or veneers, Lumineers are not an appropriate choice for esthetic veneer restorations. Dr. Engelberg suggests discussing any veneer choice with an experienced cosmetic dentist who can demonstrate an expertise in treating a variety of esthetic cases with veneers through actual before and after photos of patients treated by the dentist. Many dentists use stock photography, and the cases are not actually their own. In this situation, a patient can be one of the few (if not the first) cosmetic cases attempted by the dentist!