History of Dental Crowns
 The first civilization to use dental crowns were the Etruscans, who lived in the region that is now modern Tuscany in the 8th to 5th century B.C.. The Etruscans, who were known as Tyrrhenians by the Greeks, actually made dental crowns from ivory, bone and even human teeth. Eventually, they began to use gold for dental crowns, a practice that persists today. As early as the late 1700’s denture manufacturers discovered that porcelain-based denture teeth could be hollowed out and used to create porcelain jacket crowns. These crowns were much more esthetic than gold crowns, however they easily chipped or fractured during routine chewing, and the strength was estimated to be in the 50 MPa range. During the middle of the 20th century, the gold standard material choice for porcelain restorations became porcelain fused to metal (PFM) crowns. These restorations are exceptionally strong and durable, can withstand extreme mastication forces over long periods of time, and are relatively easily fabricated by lab technicians and seated predictably by dentists.
The first civilization to use dental crowns were the Etruscans, who lived in the region that is now modern Tuscany in the 8th to 5th century B.C.. The Etruscans, who were known as Tyrrhenians by the Greeks, actually made dental crowns from ivory, bone and even human teeth. Eventually, they began to use gold for dental crowns, a practice that persists today. As early as the late 1700’s denture manufacturers discovered that porcelain-based denture teeth could be hollowed out and used to create porcelain jacket crowns. These crowns were much more esthetic than gold crowns, however they easily chipped or fractured during routine chewing, and the strength was estimated to be in the 50 MPa range. During the middle of the 20th century, the gold standard material choice for porcelain restorations became porcelain fused to metal (PFM) crowns. These restorations are exceptionally strong and durable, can withstand extreme mastication forces over long periods of time, and are relatively easily fabricated by lab technicians and seated predictably by dentists.
A dental crown is placed for many reasons, but the most common reasons include: strengthening and restoring a decayed, broken or structurally compromised tooth, repositioning a tooth, changing the shape, contour, position, or height of a tooth, correcting occlusion, or improving esthetics. When a tooth has an existing large filling, and the tooth acquires new tooth decay, replacing that filling with an even larger filling is not a reasonable option and a crown is recommended. When a large portion of a virgin or partially restored tooth fractures, a filling is not a reasonable option and a crown is recommended. When a posterior tooth requires a root canal, a filling is not a recommended long term option as the tooth is weakened and prone to fracture without the placement of a dental crown. Finally, when several cracks appear or a tooth becomes symptomatic to chewing, a dental crown might be recommended. Many of the previously mentioned reasons for a crown revolve around improving the strength of a tooth, or improving the structural integrity of a tooth in order to avoid the possible loss of the tooth.
A crown is performed, traditionally, by preparing the tooth by removal of 0.5mm-2.0mm of tooth surface 360 degrees around the tooth to allow for room for the restorative material. Depending on the material selected, more or less removal is recommended. Gold, for example, can be very thin, and even a bit less than 0.5mm thickness, however some older porcelain materials require closer to 2.0mm of tooth structure to be removed in order to achieve sufficient strength. Once prepared, an impression of the tooth is made and sent to a dental laboratory and a temporary crown is placed to protect the tooth during the waiting period while the crown is made. At the seating appointment, the temporary crown is removed, and the definitive crown is placed over the tooth with a luting material. Patients commonly assume that a crown is permanent, however this is false—a patient can still get tooth decay and have issues in the future with the underlying tooth. Another assumption is that a patient does not have their teeth anymore, but this also is false—the patient’s tooth still remains to varying degrees below the crown.
The main focus as time has passed for cosmetic dentists has been how to achieve a natural looking restoration that can also resist failure after years of function in the oral cavity. Several attempts have come and gone, however today there are multiple options for esthetic materials to fabricate dental crowns. These materials include gold, porcelain-fused-to-gold, zirconia, feldspathic porcelain, pressed porcelain, composite, and even titanium.
The material choices are much more vast than what will be discussed, but the most common choices for Dr. Engelberg will be discussed below with a rationale for each. In addition, please refer to the resource section on porcelain veneers pages for specifics on some of these materials—it is a common misconception that porcelain used for a veneer is different than for a crown. In the hands of a skilled ceramist and restorative dentist, nearly all of the esthetic dental restorative materials can be placed successfully anywhere in the mouth in crown, onlay, inlay, or veneer form—so long as fundamental principles of occlusion, preparation and proper delivery protocols are followed.
Gold Dental Crowns
Gold is a material that has stood the test of time in dentistry, and is ideal in several ways for restoring a tooth with a dental crown. Gold will not chip, as many porcelain-based crowns can, and is considered a “soft” dental material. Soft is not something that most people associate with gold, however gold will wear away with chewing forces over time and is quite forgiving to the opposing dentition and on the tooth it is placed as well. Therefore, gold is an outstanding restorative material.
If you are interested in esthetics or cosmetic dentistry, then gold is absolutely the worst choice—very few patients elect to have any of their anterior teeth restored with gold. In addition, gold is not technically able to be bonded to the tooth, and over time the cement that is placed under a gold crown can potentially wash away, leaving voids and the potential for tooth decay.
Today, gold itself is at historic prices, and laboratories across the world have been using less gold for financial reasons. If you are interested in gold crowns, you should check to make sure that the gold that is used is “nigh noble” gold, and not “base metal” which is less costly and inferior as a restorative material. You should also prepare to pay a higher cost for high noble gold materials. Both the cost aspects and esthetic downsides to gold have pushed the dental industry to search for alternative material options for crowns.
Composite Resin Dental Crowns
Crowns can be made at a low cost with composite resin, similar to the material that is used for tooth-colored fillings. This is not currently accepted by many dentists as the standard of care, but is certainly clinically acceptable in some situations. For example, CAD/CAM machines can produce crowns out of milled blocks of composite resin (such as Paradigm) that can be used for crowns. In most cases today, however, when a crown is made from a composite material, it is used for temporary or provisional purposes.
Dr. Engelberg treats many adult reconstructive dental cases, where patients require crowns on several teeth, however they must first undergo orthodontic treatment. If a patient is at risk of a tooth fracturing, has tooth decay, or other structural issues, it makes sense to place a provitional crown made from composite material with permanent cement onto these teeth prior to orthodontic treatment. With this technique, there is little risk of complications while in braces, yet the tooth or teeth remain protected throughout that time period. The downside to this is that these crowns must be cut off after braces, and cannot usually be wiggled off with crown removers, for example.
Porcelain-Fused-to-Gold Dental Crowns
To make gold crowns more esthetic, the ability to fuse porcelain materials to gold is essential. In theory, the benefits of the “forgiving” gold and the esthetics of porcelain make a porcelain-fused-to metal crown (PFM) a potentially ideal crown. For decades, these crowns have been the most commonly prescribed crowns by dentists to laboratory technicians, and they still are very commonly prescribed today. It is easy to cement a PFM crown (they cannot be truly bonded to tooth structure), and this makes the seating appointment easy for both the patient and the dentist. As PFM’s are always metal copings with added porcelain, they are not monolithic and there is more dental laboratory labor involved.
Rising costs of gold have, unfortunately, led some dental technicians to use lesser metals under the porcelain, and it is essential that a patient be aware of the metals used in their mouth. Some dentists have even started sending their work to China (or unbeknownst to them their U.S. dental laboratory outsources their work to China), and suspect metals such as lead have been appearing in the final product. This is not to say that all technicians have stated employing these cost-cutting tactics, however it is a reality today. Dental insurance carriers reimburse dentists that are “in network” a fraction of what the price of a crown should be, sometimes as little as 40% of the fair fee. The lack of compensation must be made up somewhere, and often the lab fees are the easiest to cut—but at a substantial price to a patient receiving this often inferior dental work.
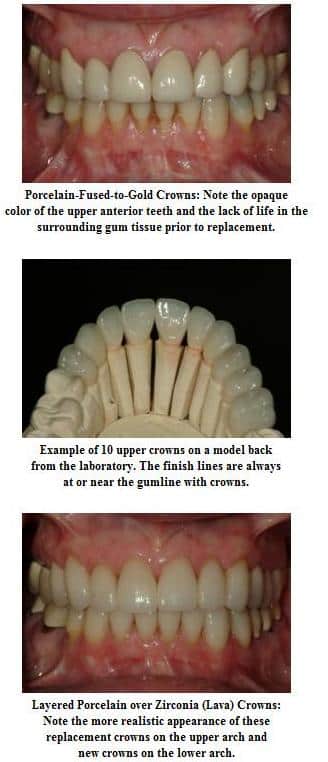 There are cosmetic downsides with PFM crowns, however, in that they are not as esthetic as all porcelain types of crowns. The metal must be blocked out with an opaque coating prior to placing the porcelain on top. The combination of the metal and layered opaquer does not allow light to pass through the crown, therefore PFM crowns typically look flat and lifeless. Some skilled technicians are able to make PFM crowns come to life in the mouth, however there are only a few ceramists that are truly capable of this, and many of these ceramists have instead chosen to fabricate crowns out of alternative materials—rather than fight the esthetic challenges of the PFM crown. Patients often complain about the black line visible around their crowns—this black line is simply a combination of visible metal and lack of light reflecting through the tooth root and gingival tissue.
There are cosmetic downsides with PFM crowns, however, in that they are not as esthetic as all porcelain types of crowns. The metal must be blocked out with an opaque coating prior to placing the porcelain on top. The combination of the metal and layered opaquer does not allow light to pass through the crown, therefore PFM crowns typically look flat and lifeless. Some skilled technicians are able to make PFM crowns come to life in the mouth, however there are only a few ceramists that are truly capable of this, and many of these ceramists have instead chosen to fabricate crowns out of alternative materials—rather than fight the esthetic challenges of the PFM crown. Patients often complain about the black line visible around their crowns—this black line is simply a combination of visible metal and lack of light reflecting through the tooth root and gingival tissue.
Zirconia Dental Crowns
Zirconia is an extraordinarily strong material, and can be layered with porcelain for a highly esthetic crown, or used to make a full-contour zirconia crown. Zirconia is technically an oxide of a metal, but most patients consider this material to be metal-free because it is white in color. There are several brands of zirconia, however 3M’s Lava is considered the most popular currently, as well as consistently high quality. Zirconia can be stained, polished, or glazed to alter the white color to best serve the shade desires of the case.
Dr. Engelberg’s 2012 article in “Dentistry Today” on the esthetics of various types of zirconia crowns is one of many on the subject of esthetics and safety of full contour zirconia crowns . The strength of zirconia is profound—no tooth colored material in dentistry is as strong. In dentistry, monolithic materials—gold, lithium disilicate, and zirconia for example are inherently more resistant to chipping, fracture, or complications. Many dental laboratories have recommended and heavily marketed inexpensive full contour (monolithic) zirconia crowns because of their extreme strength and esthetics.
Monolithic zirconia crowns are very inexpensive to make, as there is little artistry (labor) involved in making them, and they are virtually indestructible (no remakes). In addition, the ability to traditionally cement these crowns makes them easier to deliver than all porcelain crowns which must be bonded. One downside is absolutely esthetics, in that the monolithic zirconia crowns are very opaque and appear “phony” in most cases. In addition, these strong crowns are typically very difficult to remove, have an unknown wear-effect on the opposing dentition, and are difficult to adjust.
Layered zirconia crowns are actually an older invention. Prior to the arrival of the concept of monolithic zirconia crowns, the use of zirconia was as a coping or core only. A coping of zirconia is either layered with feldspathic or pressed porcelain. The concept is that one can benefit from the improved esthetics of layered porcelain while simultaneously enjoying the benefits of a high-strength zirconia core. When these crowns first were introduced, their growth was prolific because of the combination of beneficial characteristics—however many of these crowns failed. The failures were due to improper coping design and errors with the layering process, and most commonly led to chipped outer porcelain. The chips ranged from small chips on cusps or marginal ridges to complete delamination of the porcelain from the crown.
In the years that have passed, laboratory technicians have redesigned their copings so that the failure rate is much lower. Most failures are on older layered zirconia crowns that were fabricated prior to the advances now understood with regard to coping design. Today, Dr. Engelberg routinely places layered zirconia crowns, however he has replaced dozens of these crowns due to porcelain fracture. While both Dr. Engelberg and his laboratory do not charge the patient for a replacement crown, the frustration to the patient, doctor, and laboratory are apparent each time this happens. For this reason, layered zirconia crowns should only be used in the right type of patient, and are not an ideal treatment option for all patients in this author’s opinion.
Pressed Porcelain Dental Crowns
Pressing porcelain into crowns can lead to both a dramatically stronger and simultaneously beautiful restoration than any layered crown. This process is used to make porcelain veneers and the specifics of the materials involved can be found in the porcelain veneers section of the website to avoid repetition here. The premise of these crowns, however, is that a material is heated to a honey-like consistency and pressed into an investment using the lost wax technique. When the material is cooled, the result is a very strong all-porcelain crown that is monolithic. These crowns can be stained and glazed or cutback and layered for extremely esthetic results.
One downside of pressed all porcelain restorations is the more complex method of seating the restorations, especially in difficult to isolate areas of the mouth. Ideally, these crowns are adhesively bonded into place using composite resin cement, which must be done in a well-controlled dry environment. As crowns are most often placed on posterior teeth, the tongue and cheeks often provide excessive saliva contamination risks to a clean seating of these crowns. In addition, if the necessary steps are not taken to ensure that the crowns are properly bonded, microleakage can ensue and recurrent decay could be the result.
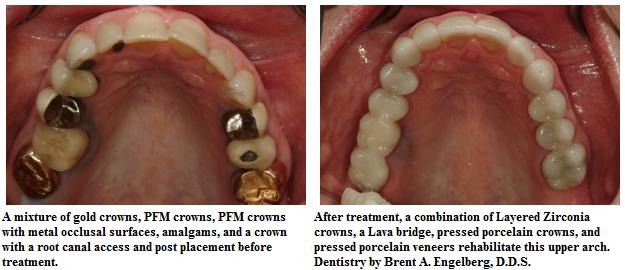
The cosmetic upsides of these crowns cannot be denied. Overall, the material choices range from highly translucent to highly opaque. In general, if a prepared tooth is a natural color, the utilization of a highly translucent pressed porcelain ingot will yield a much more esthetic result than a PFM, monolithic zirconia, and in most cases layered zirconia crown. In addition, these crowns can be carefully polished at the marginal areas to achieve an outstanding fit. There are many different types of pressed porcelain, but today lithium disilicate is the material of choice for most cosmetic dentists placing all porcelain crowns—the brand name of this material manufactured by Ivoclar Vivadent is IPS e.max. IPS e.max is about three times as strong as its predecessor, leucite-reinforced ceramic (brand name IPS Empress Esthetic).